
"Design of a successful hemianopic visual aid ideally requires that it
expands the field-of-view rather than relocate it, functions in
all positions of gaze, and avoid central diplopia."
Eli Peli, MSc, OD
inventor of the EP Horizontal Lens
Schepen's Eye Research Institute, Harvard Medical School
The EP Horizontal Lens For Hemianopsia
 The EP Horizontal Lens helps increase the functional visual field for individuals who have suffered a visual field loss from a homonymous hemianopsia. Homonymous hemianopsia frequently occur secondary to a stroke, brain trauma or brain tumor. The EP Horizontal lens works in a novel way compared to previous visual field awareness systems like the Gottlieb VFAS, Chadwick Hemianopsia Lens or InWave Lens. These traditional visual field awareness systems provide visual field expansion, but only upon the patient scanning into the edge of the system to the side. This creates a sudden image jump. The EP Horizontal lens, however, creates a simultaneous view of part of the impaired visual field. The EP Horizontal lenses are mounted in one lens on the side of the visual field loss. Either one or two EP segments may be prescribed in the carrier lens. The field expanders may be mounted either above or below the line of sight as a single system or both above and below the line of sight. This allows the patient freedom to scan back and forth horizontally throughout the lens. If the loss is on the right side of both eyes, the EP Horizontal lens is placed in the right lens. Each segment above and below eye level shifts the image inward. The brain perceptually fills in the difference between the upper and lower image.The EP Horizontal also uses higher power prism thus creating more visual field expansion than other systems.
The EP Horizontal Lens helps increase the functional visual field for individuals who have suffered a visual field loss from a homonymous hemianopsia. Homonymous hemianopsia frequently occur secondary to a stroke, brain trauma or brain tumor. The EP Horizontal lens works in a novel way compared to previous visual field awareness systems like the Gottlieb VFAS, Chadwick Hemianopsia Lens or InWave Lens. These traditional visual field awareness systems provide visual field expansion, but only upon the patient scanning into the edge of the system to the side. This creates a sudden image jump. The EP Horizontal lens, however, creates a simultaneous view of part of the impaired visual field. The EP Horizontal lenses are mounted in one lens on the side of the visual field loss. Either one or two EP segments may be prescribed in the carrier lens. The field expanders may be mounted either above or below the line of sight as a single system or both above and below the line of sight. This allows the patient freedom to scan back and forth horizontally throughout the lens. If the loss is on the right side of both eyes, the EP Horizontal lens is placed in the right lens. Each segment above and below eye level shifts the image inward. The brain perceptually fills in the difference between the upper and lower image.The EP Horizontal also uses higher power prism thus creating more visual field expansion than other systems.
The EP Horizontal concept was developed by Dr. Eli Peli of Harvard University's Schepens Eye Research Institute in 1999. Using high powered Fresnel press-on prisms, he tested this concept on an initial group of patients in his private practice with great success (Peli 2000).
Funded by National Institute of Health (NIH) Grant EY 014723, it was the subject of a national multi-center study of which our doctors at the Low  Vision Centers of Indiana participated in the clinical research. Clinical trials of the EP lens design began in 2004 at multiple sites throughout the United States. A high acceptance rate has been reported by the study.
Vision Centers of Indiana participated in the clinical research. Clinical trials of the EP lens design began in 2004 at multiple sites throughout the United States. A high acceptance rate has been reported by the study.
The results of this community based study was published in the Archives of Ophthalmology, Community-Based Trial of Peripheral Prism Visual Field Expansion Device for Hemianopia was published in the Archives of Ophthalmology in March of 2008.
"Our results demonstrate the functional utility of peripheral prism
glasses as a general mobility aid for patients with hemianopia."
Alex R. Bowers, Ph.D, Karen Keeney, MSBA, and Eli Peli, OD, Community-Based Trial of Peripheral Prism Visual Field Expansion for Hemianopia, Alex R. Bowers, Ph.D, Karen Keeney, MSBA, and Eli Peli, OD, Arch Ophthalmol, 2008 May; 126(5): 657-664.
Clinical trials have found that 12mm as an optimal separation between upper and lower prisms. An 8x22mm rounded rectangular hole is created in the carrier lens to house the prism segment(s). The carrier lens is weakened if any part of that hole is closer than 3mm to the edge of the lens.
lower prisms. An 8x22mm rounded rectangular hole is created in the carrier lens to house the prism segment(s). The carrier lens is weakened if any part of that hole is closer than 3mm to the edge of the lens.
If two segments are used a bifocal maybe placed under the lower prism but the reading area may be reduced. If only the upper segment is used, the bifocal size is not limited.
 Here a patient is fit with only the upper EP Horizontal Lens. This allows a full bifocal below. The patient reports the upper segment constantly makes her aware of walls and objects to the side of her loss from a right homonymous hemianopsia.
Here a patient is fit with only the upper EP Horizontal Lens. This allows a full bifocal below. The patient reports the upper segment constantly makes her aware of walls and objects to the side of her loss from a right homonymous hemianopsia.
The EP Horizontal lens provides a constant 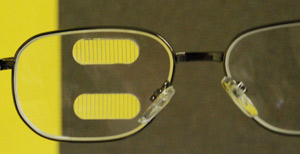 awareness of the lost field above and below the normal field of view. It also does not cause an image jump as the patient shifts in and out of the prismatic portion. The horizontal area between the two EP segments is not affected.
awareness of the lost field above and below the normal field of view. It also does not cause an image jump as the patient shifts in and out of the prismatic portion. The horizontal area between the two EP segments is not affected.
Notice in the example to the left that the yellow card which is off to the left appears in both of the EP Horizontal prism segments. The images of the yellow surface shift into the center vision. The patient’s brain learns to perceptually fill in the difference and thus the patient would appreciate that the yellow area actually runs up and down the left side.
The patient can move their eye back and forth without the image jump that occurs with other field expanders. The concept that the brain can see the central horizontal portion simultaneously view the prismatic images is called multiplexing. The concept of multiplexing in low vision care has been pioneered by Dr. Peli.
Please contact us if you have any questions.
The Low Vision Centers of Indiana
Richard L. Windsor, O.D., F.A.A.O., D.P.N.A.P.
Craig A. Ford, O.D., F.A.A.O.
Laura K. Windsor, O.D., F.A.A.O.
Ali E. Prible, O.D.
Indianapolis (317) 844-0919
Fort Wayne (260) 432-0575
Hartford City (765) 348-2020